
Maigan Espinili Maruquin
Introduction
Cats, as a fur family, require health attention. However, some felines can get infected with certain types of inherited diseases. One of the most prevalent genetic diseases is the Feline Polycystic Kidney Disease (PKD) [1, 2], which causes the progressive development of multiple fluid-filled cysts in the kidney and in some cases extends to the liver and pancreas [2-5]. Prevalence of the PKD in Persian cats has been studied in different countries including, the United Kingdom (49.2%) [6], Japan (46%) [7], Australia (45%) [8], and France (40.45%) [9]. Reports suggest that the disease is not related to the sex of the feline, after results show no statistical differences between males and females [9, 10]. Different species of felines can get the said disease like Charteux [11], Neva Masquerade cat [12], and Scottish Fold and American Shorthair [7], however, it is most commonly inherited by the Persian and Persian- related breeds [3] with 35 to 57% detection via ultrasonography or genetic testing [13]. It is suspected that all the feline breeds could have inherited the mutation where the disease starts, considering that around 80% of all current feline breeds have had some type of cross with Persian breed [3, 14].
In humans, 1 in 500–1000 of the general population can inherit Autosomal dominant polycystic kidney disease (ADPKD) [15], which is characterized by increase in kidney size caused by the development and progressive enlargement of renal cysts, eventually leading to a steady decline in glomerular filtration rate [16]. The PKD1 and PKD2 genes, which are responsible for coding the polycystin-1 and 2 proteins, where 85 % and 15%, respectively, are responsible for the mutations [17].
Relative to the cases recorded with ADPKD in cats, the feline ortholog of the human PKD1 gene, which is also named PKD1, were recorded to have a single germline mutation. During the mutation, at exon 29 of the feline PKD1 gene, position 3284, a pyrimidine base (cytosine, C) is substituted by a purine base (adenine, A), wherein the premature stop codon produced causes the 25% loss in the C- Terminal formation of polycystin-1 protein [3, 18, 19]. With similar features clinically and morphologically in both human and feline ADPKD [2], feline PKD is a good representation for human ADPKD [7].
Clinical Presentations
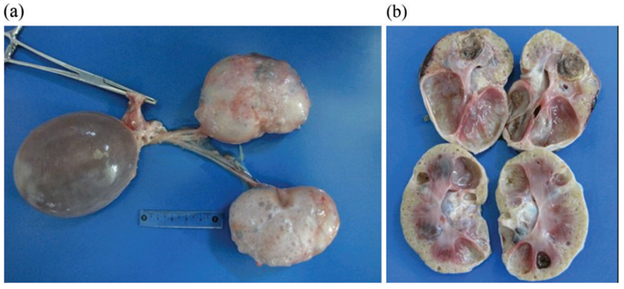
Fig. 1. Postmortem images, including cross-section of the polycystic kidneys of a seven-year-old, entire male British shorthair cat (cat 4), tested positive for the PKD1 mutation, demonstrating multiple cysts of variable sizes in both kidneys (a, b). [4]
The polycystin-1 is suggested to play a role in cell–cell and matrix–cell interactions [20]. The primary cilium, where this protein is expressed, functions in fluid transport and chemo and mechanoreceptors [21, 22].
Cysts of different sizes were presented in renal cortex and medulla, sometimes occurs in the liver and pancreas, as well [8], and increases both in size and quantity as they age [23]. With slow growth and progression, affected cats start to deteriorate renal functions [7]. The cysts develop by different scenarios including the increase of cell proliferation, fluid secretion, and extracellular matrix alterations, cilia with lost polarization would then alter the water reabsorption function [3, 24]. Secondary to renal cysts development, obstruction due to nephrolithiasis, lymphoma and chronic kidney disease with interstitial nephritis are also displayed, especially in old cats [8, 25]
In a study conducted among cats in Turkey, some diagnosed cats were reported for fatigue, anorexia, and vomiting. During palpation, an increase in total kidney volume was discovered, and cystic lesions were seen in the cortex of both kidneys when ultrasonography was performed [19].
Generally, apathy, anorexia, weight loss, bad appearance of the coat, polyuria and polydipsia, and gastrointestinal disorders could be observed [26-28], while general dehydration and pale mucous membranes are also noticeable on clinical examinations [3].
Elevated serum Cre concentration has been presented as one of the clinical signs in cats from three years old, while other cats at nine showed normal concentration. This suggests variable clinical courses of the disease [7]. Whereas, few cases showed hepatic cysts an extrarenal manifestation [6].
Diagnosis
Imaging Diagnosis
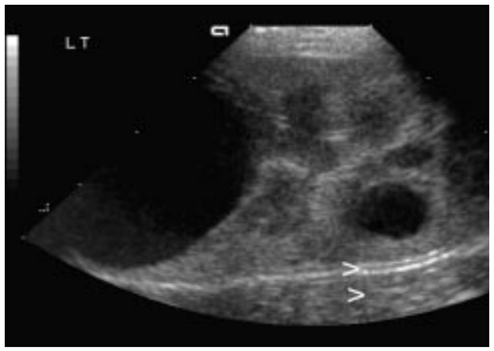
Fig. 2. Ultrasound picture of a 2.5 year old Persian cat, positive for PKD. Note the distal enhancement beyond the anechoic cyst structures (arrow). The largest cyst measures 29 mm in diameter [8].
The Ultrasound is known to be with the highest successful diagnosis, allowing quick and reliable diagnosis [23], and is considered due to availability and non-invasive, safe, cheap and effectivity in detecting the presence of kidney cysts [28]. Whereas, radiography and intravenous urography are usually used in more advanced cases, like when there is a presence of multiple, large cysts [3].
Molecular Approach
Various PCR methods have been used to identify and amplify the DNA fragment of interest [3]. The RFLP-PCR was developed and used [18], real-time PCR or quantitative PCR is known to be reliable and faster than the earlier technique [29]. Whereas, ARMS-PCR (Amplification-refractory mutation system-Polymerase Chain Reaction) presented its advantages in time, low quantity of samples needed and its low cost, which has resulted in 100% sensitivity and specificity [30].
The synergistic use of genetic testing to confirm the presence of the causal mutation and make an early diagnosis; and the ultrasound to diagnose polycystic kidney disease and to monitor the progression of the disease has been agreed by several authors to plan detection programs for feline PKD [3, 30-32].
For as early as three years old, affected felines can develop signs of impaired renal function, and thus, positive cats are strongly discouraged for breeding [7].
References
- Young, A.E., et al., Feline polycystic kidney disease is linked to the PKD1 region. Mamm Genome, 2005. 16(1): p. 59-65.
- Eaton, K.A., et al., Autosomal dominant polycystic kidney disease in Persian and Persian-cross cats. Vet Pathol, 1997. 34(2): p. 117-26.
- Schirrer, L., P.J. Marín-García, and L. Llobat, Feline Polycystic Kidney Disease: An Update. 2021. 8(11): p. 269.
- Nivy, R., et al., Polycystic kidney disease in four British shorthair cats with successful treatment of bacterial cyst infection. 2015. 56(9): p. 585-589.
- Bosje, J.T., T.S. van den Ingh, and J.S. van der Linde-Sipman, Polycystic kidney and liver disease in cats. Vet Q, 1998. 20(4): p. 136-9.
- Cannon, M.J., et al., Prevalence of polycystic kidney disease in Persian cats in the United Kingdom. 2001. 149(14): p. 409-411.
- Sato, R., et al., Epidemiological evaluation of cats associated with feline polycystic kidney disease caused by the feline PKD1 genetic mutation in Japan. Journal of Veterinary Medical Science, 2019. advpub.
- BECK, C. and R. LAVELLE, Feline polycystic kidney disease in Persian and other cats: a prospective study using ultrasonography. 2001. 79(3): p. 181-184.
- Barthez, P., P. Rivier, and D. Begon, Prevalence of polycystic kidney disease in Persian and Persian related cats in France. 2003. 5(6): p. 345-347.
- BARRS, V., et al., Prevalence of autosomal dominant polycystic kidney disease in Persian cats and related-breeds in Sydney and Brisbane. 2001. 79(4): p. 257-259.
- Volta, A., et al., Polycystic kidney disease in a Chartreux cat. J Feline Med Surg, 2010. 12(2): p. 138-40.
- Jasik, A. and M. Kulesza, Polycystic kidney disease in a Neva Masquerade cat. 2014. 55(7): p. 387-387.
- Chew, D.J., DiBartola, S. P. & Schenck, P. A., Familial renal diseases of dogs and cats. In: Canine and Feline Nephrology and Urology, 2011. 2nd edn: p. 197-217.
- Scalon, M.C., et al., Touchdown polymerase chain reaction detection of polycystic kidney disease and laboratory findings in different cat populations. 2014. 26(4): p. 542-546.
- Spithoven, E.M., et al., Renal replacement therapy for autosomal dominant polycystic kidney disease (ADPKD) in Europe: prevalence and survival–an analysis of data from the ERA-EDTA Registry. Nephrol Dial Transplant, 2014. 29 Suppl 4(Suppl 4): p. iv15-25.
- Torres, V.E., P.C. Harris, and Y. Pirson, Autosomal dominant polycystic kidney disease. Lancet, 2007. 369(9569): p. 1287-1301.
- Al-Bhalal, L. and M. Akhtar, Molecular Basis of Autosomal Recessive Polycystic Kidney Disease (ARPKD). 2008. 15(1): p. 54-58.
- Lyons, L.A., et al., Feline polycystic kidney disease mutation identified in PKD1. J Am Soc Nephrol, 2004. 15(10): p. 2548-55.
- Bilgen, N., et al., Prevalence of PKD1 gene mutation in cats in Turkey and pathogenesis of feline polycystic kidney disease. 2020. 32(4): p. 549-555.
- Frazier, R.L. and A.R.J.A.P. Huppmann, Educational Case: Autosomal Dominant Polycystic Kidney Disease. 2020. 7: p. 2374289520939257.
- Braun, W.E.J.C.C.j.o.m., Autosomal dominant polycystic kidney disease: emerging concepts of pathogenesis and new treatments. 2009. 76(2): p. 97-104.
- Noel, N., P.J.N. Rieu, and Therapeutique, Pathophysiology, epidemiology, clinical presentation, diagnosis and treatment options for autosomal dominant polycystic kidney disease. 2015. 11(4): p. 213-225.
- Yu, Y., et al., Kidney and cystic volume imaging for disease presentation and progression in the cat autosomal dominant polycystic kidney disease large animal model. 2019. 20(1): p. 1-11.
- Sharma, M., G.A. Reif, and D.P. Wallace, In vitro cyst formation of ADPKD cells, in Methods in Cell Biology. 2019, Elsevier. p. 93-111.
- Kappe EC, H.W., Gerwing M, et al., Polycystic kidney disease in the German population of Persian cats. A comparative study of ultrasonographical examination and
genetic testing. Tierarztl Prax Ausg K, 2005(33): p. 413–418.
- Battershell, D. and J.P. Garcia, Polycystic kidney in a cat. J Am Vet Med Assoc, 1969. 154(6): p. 665-6.
- Bergmann, C.J.P.N., ARPKD and early manifestations of ADPKD: the original polycystic kidney disease and phenocopies. 2015. 30(1): p. 15-30.
- Guerra, J.M., et al., Age-based ultrasonographic criteria for diagnosis of autosomal dominant polycystic kidney disease in Persian cats. 2019. 21(2): p. 156-164.
- Helps, C., et al., Correlation of the feline PKD1 genetic mutation with cases of PKD diagnosed by pathological examination. 2007. 83(2): p. 264-268.
- Lee, Y.-J., et al., Molecular detection of autosomal-dominant feline polycystic kidney disease by multiplex amplification refractory mutation system polymerase chain reaction. 2010. 22(3): p. 424-428.
- Gluecksmann-Kuis, M., et al., Polycystic kidney disease: the complete structure of the PKD1 gene and its protein. 1995. 81(2): p. 289-298.
- Bonazzi, M., et al., Comparison between ultrasound and genetic testing for the early diagnosis of polycystic kidney disease in Persian and Exotic Shorthair cats. 2009. 11(6): p. 430-434.