
Factors That Affect Veterinary Antibiotic Ranking and Usage

Table of Contents 1. Introduction: Why Antibiotic Ranking Matters Defining Antibiotic Rank Antibiotic ranking, exemplified by frameworks such as the Desirability of Outcome Ranking for the Management of Antimicrobial Therapy (DOOR MAT), is a comparative evaluative system used to classify antibiotics based on clinical, microbiological, and stewardship-related outcomes. These ranking models integrate multiple criteria to provide a balanced assessment of antibiotic desirability and therapeutic appropriateness. Drawing from these frameworks, antibiotic ranking generally incorporates four key dimensions: Clinical Effectiveness or Activity:The ranking prioritizes treatments containing an active agent against the infecting pathogen. The DOOR MAT framework, for instance, evaluates whether a therapeutic choice is active or inactive against a confirmed organism, directly linking activity with patient outcomes. Resistance Rates and Spectrum of Activity:Ranking methods also consider the relationship between antimicrobial spectrum and resistance potential. Narrow-spectrum antibiotics, such as penicillin V, amoxicillin, and dicloxacillin, are typically ranked higher in desirability because they exert less selective pressure on the microbiota. In contrast, broad-spectrum agents, including third-generation cephalosporins (e.g., ceftriaxone), fluoroquinolones (e.g., ciprofloxacin, levofloxacin), and carbapenems (e.g., meropenem), tend to rank lower due to their greater ecological impact and higher risk of promoting resistance. Frameworks like the Antibiotic Spectrum Index (ASI) quantify these differences by assigning spectrum scores to each agent, enabling objective comparison and stewardship-based decision-making. Safety Profile and Cost Considerations:Although not always included in the primary ranking score, additional factors—such as toxicity, cost, availability, ease of administration, and drug–drug interactions—inform antibiotic appropriateness. For example, antibiotics within the WHO “Access” category are generally considered safer and more affordable options. Stewardship Importance:Ranking frameworks also evaluate antibiotics based on their role in antimicrobial stewardship, emphasizing the use of agents that balance clinical efficacy with the minimization of resistance development. The Role of Antibiotic Ranking in Clinical and Policy Decisions Antibiotic ranking systems are essential tools in clinical governance and global health policy, particularly in addressing the growing threat of antimicrobial resistance (AMR). Guiding Treatment Guidelines and Formulary Decisions:Ranking methods provide a structured and quantitative means of assessing antibiotic appropriateness. They assist institutional committees in developing treatment protocols by integrating local surveillance data, such as antibiograms, to match antibiotic selection with resistance profiles. The guiding principle is to ensure that antibiotic therapy—when justified—is both targeted and evidence-based. Narrow-spectrum agents are therefore prioritized over broad-spectrum alternatives whenever clinical efficacy is maintained. Informing AMR Policy and Stewardship Programs:Because 30% to 50% of antibiotic prescriptions are considered inappropriate, ranking frameworks are vital for identifying and reducing misuse. They help stewardship teams evaluate prescribing patterns and adjust therapeutic choices to minimize selective pressure on bacterial populations. Global policy initiatives, such as the WHO’s Access, Watch, Reserve (AWaRe) classification, further support the rational distribution of antibiotic use. Similarly, the WHO Bacterial Priority Pathogens List (BPPL) ranks pathogens based on their resistance threat, thereby guiding research and development (R&D) priorities for new antimicrobials. The WHO AWaRe Classification: A Model of Stewardship-Based Ranking The WHO AWaRe Classification, launched in 2017, is a globally recognized model designed to improve antibiotic use and curb resistance by categorizing antibiotics according to their public health importance and resistance risk. The system divides antibiotics into three stewardship-based categories: Access:These antibiotics pose a lower risk of resistance and are recommended as first- or second-line treatments for common infections. They are typically safe, affordable, and suitable for wide availability without restriction. Watch:Broad-spectrum agents associated with higher resistance potential fall into this group. Their use should be limited to specific indications or cases where Access antibiotics are ineffective. Reserve:These represent last-resort antibiotics reserved for infections caused by multidrug-resistant organisms. Their use should be tightly controlled and guided by expert consultation. The WHO recommends that more than 60% of national antibiotic consumption should derive from the Access group. The WHO recommends that more than 60 percent of national antibiotic consumption should come from the Access group. Organizations such as the Global Antibiotic Research and Development Partnership (GARDP) have proposed refinements to the AWaRe framework, particularly regarding Reserve antibiotics, to keep the system clinically relevant and responsive to evolving global resistance patterns. 2. Clinical Efficacy and Spectrum of Activity Broad vs. Narrow Spectrum: How Therapeutic Coverage Shapes Rank Antibiotic ranking frameworks prioritize therapeutic coverage based on the dual goals of effective patient treatment and antimicrobial stewardship. The general preference is for narrow-spectrum agents over broad-spectrum agents, provided that patient outcomes are not compromised. Key aspects of how spectrum shapes rank include: Minimizing Selective Pressure:Effective stewardship requires evaluating not only the efficacy of an antibiotic but also its spectrum of activity to minimize selective pressure, which drives the emergence of future resistance. Defining Desirability:Frameworks such as the Desirability of Outcome Ranking for the Management of Antimicrobial Therapy (DOOR MAT) classify treatment selection according to two primary principles: Treatments containing an active agent are more desirable than inactive ones; and Narrow-spectrum antibiotics are more desirable than broad-spectrum agents when equally effective. Ranking Overtreatment:In systems such as DOOR MAT, inappropriate therapy is defined as treatment that is active but unnecessarily broad in spectrum, known as overtreatment. Overtreatment is stratified into ordered categories, such as slight overtreatment, moderate overtreatment, and severe overtreatment. All of these rank lower than ideal treatment, which is the narrowest active therapy. Quantitative Measurement:The Antibiotic Spectrum Index (ASI) provides a quantitative measure of antibiotic exposure based on spectrum of activity. Each antibiotic receives a score from 1 to 13, allowing classification into four categories: Narrow (1–2), Intermediate (3–4), Broad (5–7), and Very Broad (≥8).Studies using ASI have shown that the mean ASI increases with the level of care, rising from Narrow in outpatients to Broad and Very Broad in hospitalized or ICU patients, illustrating the link between clinical setting and antibiotic breadth. Mechanism of Action: Bactericidal vs. Bacteriostatic Distinction The mechanism of action determines an antibiotic’s pharmacological effect on its target pathogen and is a major factor influencing its ranking and clinical appropriateness. General Mechanism:Antibiotics are selectively cytotoxic to microbial cells. They typically act either by disrupting the peptidoglycan cell wall or by interfering with essential metabolic processes within the bacterial
Feline Herpesvirus 1 (FHV-1) Infection

Bioguard Corporation Feline herpesvirus-1 (FHV-1) is a common viral infection in cats that primarily affects the upper respiratory system. It is a major cause of feline viral rhinotracheitis (FVR), which presents symptoms like sneezing, nasal discharge, and conjunctivitis (eye inflammation). FHV-1 is highly contagious among cats and is spread through direct contact with infected saliva, eye or nasal secretions, or contaminated environments. Once infected, many cats can become lifelong carriers of the virus, with symptoms reoccurring during times of stress or illness. Transmission A cat can become infected with this virus through direct exposure to viral particles. The virus is transmitted through saliva, as well as eye and nasal discharges from an infected cat. Infection occurs when a susceptible cat comes into contact with an infected cat or with contaminated objects, such as clothing, food and water bowls, or furniture that carry the viral particles. Though the virus is fragile in the environment and doesn’t survive for long outside the host, it remains a significant concern because many cats become lifelong carriers after infection. Even when no symptoms are present, stress or illness can trigger a flare-up, allowing the carrier to shed the virus and infect others. Incubation Period of FHV-1 Infection After a cat is infected with FVR, symptoms typically appear within two to five days, which is the incubation period of the disease. During this time, the cat can already infect other cats. Once symptoms develop, the active infection usually lasts about 10 to 20 days. Clinical Signs Upper respiratory signs of FVR include sneezing, nasal discharge, fever, loss of appetite, and coughing. Eye-related symptoms may encompass discharge, conjunctivitis or chemosis, changes in color, and corneal ulcers. In severe cases, the skin around the face may show signs such as redness, swelling, crusting, and hair loss. Other non-specific symptoms can include fever, lethargy (tiredness), anorexia (poor appetite), and enlarged lymph nodes. Diagnosis In most cases, a specific diagnosis of FHV infection is not necessary. A presumptive diagnosis of FVR is based primarily on a cat’s medical history and clinical signs combined with the findings on physical examination, particularly if the cat has evidence of a corneal infection. Corneal staining with fluorescein dye is often performed to look for any ulcers that may have developed. However, if a specific diagnosis is needed, ocular or oral swabs can be sent to a veterinary lab. There, the virus can be cultured or, more commonly detected by PCR. Additionally, evidence of the virus can be found in biopsies, which can help diagnose FHV-associated dermatitis. Prevention Preventing FVR involves several key strategies: Vaccination: Core vaccines for cats include the FVR vaccine, which significantly reduces the severity and duration of the illness, even if it doesn’t completely prevent infection. Hygiene and Sanitation: Good hygiene practices, such as washing your hands thoroughly before and after handling other cats, can help prevent the spread of FHV-1. Keeping your cat’s living environment clean is also important. Minimizing Stress: Stress can trigger the reactivation of the virus in carrier cats. Providing a stable, stress-free environment can help reduce the likelihood of outbreaks. Isolation: If the cat is infected, keeping her isolated from other cats can prevent the spread of the virus. This is especially important in multi-cat households, boarding facilities, and shelters. References Bergmann M, Speck S, Rieger A, et al. Antibody response to feline herpesvirus-1 vaccination in healthy adult cats. J Feline Med Surg. 2020 Apr;22(4):329-338. Cottingham E, Johnstone T, Hartley CA, et al. Update on feline alphaherpesvirus-1 seroprevalence in Victorian feral and owned cats. Aust Vet J. 2022 May;100(5):187-189. Thomasy SM, Maggs DJ. A review of antiviral drugs and other compounds with activity against feline herpesvirus type 1. Vet Ophthalmol. 2016 Jul;19 Suppl 1(Suppl 1):119-30.
What Does “Antibiotic Rank” Mean in Veterinary Medicine?
Table of Contents 1. Why “Antibiotic Rank” Matters in Veterinary Medicine Defining antibiotic ranking in veterinary antimicrobial stewardship In veterinary antimicrobial stewardship, antibiotic ranking refers to the structured classification of antimicrobial agents based on their public health importance, therapeutic value in animals, and the potential risk they pose for driving antimicrobial resistance. These ranking systems create a shared scientific framework that identifies which antibiotics should be preserved, which require caution, and which remain suitable as first-line options for veterinary use. International authorities guide this process. The World Organisation for Animal Health (WOAH, formerly OIE) publishes a List of Antimicrobial Agents of Veterinary Importance, while the European Medicines Agency’s Antimicrobial Advice Ad Hoc Expert Group (AMEG) categorizes antibiotics into risk-based groups intended to harmonize stewardship across the European Union. Collectively, these systems promote the rational and judicious use of antimicrobials in animals. How ranking frameworks help veterinarians choose antibiotics responsibly Antibiotic ranking systems function as practical decision tools for veterinarians. By stratifying antimicrobials according to their criticality, these frameworks: Highlight drugs that require strict restraint Direct clinicians toward lower-risk first-line options Support evidence-based prescribing For example, the AMEG classification guides veterinarians by designating high-risk agents in Category B (Restrict), which should only be used when no suitable alternatives exist. This structured hierarchy helps balance animal welfare with the responsibility to limit the emergence of antimicrobial resistance. One Health context: linking animal use to human and environmental resistance risks Antibiotic ranking is fundamentally shaped by the One Health perspective, which recognizes that the health of humans, animals, and the environment forms an interconnected system. Antimicrobial use in animals can influence resistance patterns in human pathogens through several pathways, including food production, environmental contamination, and direct human–animal interactions. Because antibiotic use in one sector can amplify resistance risks across the entire ecosystem, global organizations emphasize the need for coordinated stewardship across species. Updated scientific opinions, such as those issued by the EMA’s AMEG or WOAH’s expert panels, explicitly address how antibiotic choices in veterinary medicine affect both animal health and public health. In this context, responsible prescribing in animals becomes an essential contribution to preserving the long-term effectiveness of antimicrobial agents worldwide. (European Medicines Agency & AMEG, 2024; World Organisation for Animal Health, 2021). 2. What “Antibiotic Rank” Means in Veterinary Medicine In veterinary medicine, antibiotic ranking refers to the structured classification of antimicrobial agents based on their therapeutic importance, public health relevance, and the potential risks associated with their use. These systems create a risk-based categorization framework that guides veterinarians in the rational use of antimicrobials across all animal sectors. International bodies have established standardized frameworks to support responsible prescribing. The WOAH (formerly OIE) List of Antimicrobial Agents of Veterinary Importance and the AMEG classification are two of the most widely recognized systems. Both frameworks rely on specific scientific criteria to determine how antibiotics should be prioritized for use in animals. Key Criteria Used in Veterinary Antibiotic Ranking Public health importance of the antibiotic classRanking systems evaluate how the use of a particular antimicrobial in animals may affect human health. Antibiotic classes that are critically important to human medicine are placed into higher-risk categories, emphasizing that their veterinary use should be limited and carefully justified. Risk of resistance transfer to humansAntimicrobial resistance moves across species, ecosystems, and food systems. Ranking frameworks incorporate the likelihood that resistance genes selected in animals could reach human populations through direct contact, the food chain, or environmental pathways. AMEG specifically provides updated scientific advice that incorporates risks to both public health and animal health. Therapeutic necessity in animalsSome antimicrobial classes are essential for maintaining animal welfare. The WOAH list identifies drugs of clear veterinary importance, recognizing that certain infections in livestock and companion animals cannot be effectively managed without them. Ranking systems balance this therapeutic need with the potential broader risks associated with drug use. • Availability of suitable alternativesAntibiotic ranking promotes responsible antimicrobial selection by encouraging the use of lower-risk alternatives whenever they provide adequate therapeutic benefit. By defining clear categories, frameworks help veterinarians reserve higher-risk or human-critical agents for cases where no appropriate alternatives exist, supporting the rational use of antimicrobials in daily practice. 3. Understanding the EMA AMEG Antibiotic Categorization System The Antimicrobial Advice Ad Hoc Expert Group (AMEG) of the European Medicines Agency (EMA) defines a risk-based antibiotic categorization system that guides the prudent and responsible use of antimicrobials in animals. This system evaluates both the public health consequences of antimicrobial resistance (AMR) arising from veterinary use and the therapeutic necessity of these drugs for maintaining animal health. AMEG stratifies antimicrobials into four categories, ranging from A to D, with Category A representing the highest public health risk and Category D representing the lowest. Category Risk Level / AMEG Meaning Veterinary Directive Examples of Antibiotic Classes Use Context Category A – Avoid Highest risk, reserved exclusively for human medicine Not authorized for veterinary use in the EU. May only be used in companion animals in exceptional cases and only under the prescribing cascade. Absolutely prohibited in food-producing animals. Carbapenems (meropenem, doripenem), glycopeptides (vancomycin), oxazolidinones (linezolid), select advanced cephalosporins/penems reserved for human therapy. Human-only antibiotics where veterinary use could severely compromise public health. Category B – Restrict Critically important for human medicine Use only when no effective Category C or D alternatives exist. Veterinary use must be justified. Diagnostic requirement: Antimicrobial susceptibility testing (AST) recommended before use. Fluoroquinolones (enrofloxacin, marbofloxacin), 3rd–4th gen cephalosporins (ceftiofur, cefquinome), polymyxins (colistin, polymyxin B). Category C – Caution Medium risk; human alternatives available but limited veterinary alternatives Use only when Category D drugs would not provide adequate clinical efficacy. Macrolides (tylosin, tulathromycin), aminoglycosides except spectinomycin (gentamicin, streptomycin), 1st–2nd gen cephalosporins, aminopenicillins with β-lactamase inhibitors (amoxicillin–clavulanic acid). Provides options for cases where first-line agents may be ineffective. Category D – Prudence Lowest public-health risk Recommended as first-line options when clinically appropriate. Avoid overuse, long treatment durations, and routine group treatments unless individual treatment is not feasible. Penicillins (amoxicillin, benzylpenicillin), tetracyclines (oxytetracycline, doxycycline), sulfonamides including potentiated combinations (sulfadiazine + trimethoprim).
Understanding Antibiotic Classifications: A Comprehensive Guide
Antibiotics are essential tools in modern medicine, used to combat bacterial infections that could otherwise lead to severe health issues or even death. To use these powerful drugs effectively, it’s crucial to understand the different classifications of antibiotics, which are based on their chemical structure, mechanism of action, and spectrum of activity. This article explores the main classifications of antibiotics, providing an overview of their uses and how they work. Beta-Lactam Antibiotics Examples: Penicillins, Cephalosporins, Carbapenems, Monobactams Mechanism of Action: Beta-lactam antibiotics work by inhibiting the synthesis of bacterial cell walls. They target the penicillin-binding proteins (PBPs) that are crucial for forming peptidoglycan, a key component of the bacterial cell wall. By disrupting this process, beta-lactams weaken the bacterial cell wall, leading to cell lysis and death. Uses: These antibiotics are widely used to treat a variety of infections, including respiratory tract infections, urinary tract infections, skin infections, and more. Penicillins are often the first line of defense against many common bacterial infections. Macrolides Examples: Erythromycin, Azithromycin, Clarithromycin Mechanism of Action: Macrolides inhibit bacterial protein synthesis by binding to the 50S ribosomal subunit, preventing the translocation of peptides. This action effectively stops the bacteria from growing and multiplying. Uses: Macrolides are particularly useful for treating respiratory infections, such as pneumonia and bronchitis, as well as skin infections. They are also an alternative for patients allergic to penicillin. Tetracyclines Examples: Tetracycline, Doxycycline, Minocycline Mechanism of Action: Tetracyclines inhibit bacterial protein synthesis by binding to the 30S ribosomal subunit. This prevents the attachment of aminoacyl-tRNA to the mRNA-ribosome complex, thereby halting protein synthesis and bacterial growth. Uses: Tetracyclines are used to treat a variety of infections, including skin infections, respiratory tract infections, and urinary tract infections. Aminoglycosides Examples: Gentamicin, Amikacin, Tobramycin Mechanism of Action: Aminoglycosides bind to the 30S subunit of bacterial ribosomes, leading to the misreading of mRNA. This causes the bacteria to produce faulty proteins, ultimately leading to cell death. Uses: These antibiotics are often used to treat serious infections caused by Gram-negative bacteria, such as sepsis, endocarditis, and complicated urinary tract infections. Due to their potential for toxicity, they are usually reserved for severe infections. Fluoroquinolones Examples: Ciprofloxacin, Levofloxacin. Mechanism of Action: Fluoroquinolones inhibit bacterial DNA gyrase and topoisomerase IV, enzymes critical for DNA replication and transcription. By disrupting these processes, fluoroquinolones prevent bacterial cell division and lead to cell death. Uses: Fluoroquinolones are used to treat a variety of infections, including respiratory tract infections, urinary tract infections, gastrointestinal infections, and skin infections. Sulfonamides Examples: Sulfamethoxazole, Sulfadiazine Mechanism of Action: Sulfonamides inhibit dihydropteroate synthase, an enzyme involved in folate synthesis in bacteria. Folate is necessary for DNA synthesis and cell division, so its inhibition leads to bacterial growth arrest. Uses: Sulfonamides are commonly used in combination with trimethoprim (e.g., as co-trimoxazole) to treat urinary tract infections, respiratory infections, and some types of diarrheas. Glycopeptides Examples: Vancomycin Mechanism of Action: Glycopeptides inhibit bacterial cell wall synthesis by binding to the D-alanyl-D-alanine termini of cell wall precursor units. This prevents the cross-linking of peptidoglycan chains, which is essential for bacterial cell wall strength and rigidity. Uses: Glycopeptides are used primarily to treat serious Gram-positive infections, especially those caused by methicillin-resistant Staphylococcus aureus (MRSA) and other resistant organisms. Oxazolidinones Examples: Linezolid, Tedizolid Mechanism of Action: Oxazolidinones inhibit protein synthesis by binding to the 50S subunit of the bacterial ribosome, preventing the formation of a functional initiation complex for protein translation. Uses: Oxazolidinones are used to treat serious infections caused by Gram-positive bacteria, including MRSA and vancomycin-resistant enterococci (VRE).
Fowl Pox

Bioguard Corporation Fowl pox is a slow-spreading viral disease affecting chickens, turkeys, and various other birds. It is characterized by proliferative skin lesions that develop into thick scabs (cutaneous form) and lesions in the upper respiratory and digestive tracts (diphtheritic form). A presumptive diagnosis can be made in the field based on distinctive skin lesions, but confirmation requires detecting cytoplasmic inclusion bodies in affected cells. Etiology Fowl pox has a world-wide distribution and is caused by a DNA virus of the genus Avipoxvirus of the family Poxviridae. Virions are somewhat pleomorphic, generally brick-shaped (220–450 nm long×140–260 nm wide×140–260 nm thick) with a lipoprotein surface membrane displaying tubular or globular units (10–40 nm). The large DNA virus is resistant and may survive in the environment for extended periods in dried scabs. Avipoxvirus affecting more than 230 species in 23 orders of wild and domesticated birds. Within the Avipoxvirus genus there are currently 10 recognized species: : Fowlpox virus, Canarypox virus, Juncopox virus, Mynahpox virus, Psittacinepox virus, Sparrowpox virus, Starlingpox virus, Pigeonpox virus, Turkeypox virus, and Quailpox virus, according to the International Committee on Taxonomy of Viruses. Transmission The fowl pox virus is abundant in lesions and typically spreads through contact with skin abrasions. Scabs shed from recovering birds in poultry houses can become airborne, leading to infection. Mosquitoes and other biting insects can also act as mechanical vectors, rapidly spreading the virus when mosquitoes are prevalent. The virus is highly resistant in dry scabs, making it easy to transmit to uninfected birds. Fowl pox can affect birds of any age and may occur year-round. Clinical signs Clinical signs are somewhat variable depending on the host species, virulence of the virus strain, distribution of lesions, and other complicating factors. In chickens and turkeys, signs may vary with two overlapping forms of the disease: Cutaneous (dry pox): The dry form begins with a pimple or scab on non-feathered areas of the skin such as the comb, wattles, eyelids, feet, and legs. Eventually, the infection may spread to other feathered areas of the body. Infected birds often have difficulty eating and reduced feed intake and weight loss is common. Cutaneous lesions on the eyelids may cause complete closure of one or both eyes. Diphtheritic (wet pox): The wet form produces diphtheritic, yellow canker lesions on oral mucous membranes, tongue, esophagus, or trachea. Lesions in the upper digestive and respiratory tract may result in inappetence and dyspnea, respectively. Other mild to severe respiratory signs may also occur. Lesions in the eye and nasal cavity lead to ocular or nasal discharges. Diagnosis: A presumptive diagnosis can be made in the field based on characteristic skin lesions. The diagnosis should be confirmed by laboratory testing. Microscopic examination of affected tissue sections stained with H&E reveals eosinophilic cytoplasmic inclusion bodies. Inclusions are also detected by fluorescent antibody and immunoperoxidase methods. Viral particles, with typical poxvirus morphology, can be detected by electron microscopy. The virus can be isolated in the chorioallantoic membrane (CAM) of chicken embryos, susceptible birds, or avian cell cultures. Field viruses can be detected in the laboratory by polymerase chain reaction (PCR). Prevention and Control Fowl pox and pigeon pox live virus vaccines are commonly used for immunization of chickens. Vaccination effectively prevents the disease and may limit spread within actively infected flocks. No treatment exists for birds infected with avian pox viruses. References Giotis ES, Skinner MA. Spotlight on avian pathology: fowlpox virus. Avian Pathol. 2019 Apr;48(2):87-90. Molini U, Mutjavikua V, de Villiers M et al. Molecular characterization of avipoxviruses circulating in Windhoek district, Namibia 2021. J Vet Med Sci. 2022 May 25;84(5):707-711.
Factor VII Deficiency in Dogs

Bioguard Corporation Canine Factor VII (FVII) deficiency is an autosomal recessive genetic disorder that leads to a mild to moderate blood clotting problem in affected dogs. Puppies with the condition may exhibit symptoms such as nosebleeds (epistaxis) and gum bleeding, while adult dogs are more prone to bruising and skin issues like dermatitis. Though bleeding episodes tend to decrease in severity as the dog matures, the disorder still causes ongoing issues throughout the animal’s life. FVII deficiency was first identified in the Migluo breed. Most dogs are diagnosed when they visit a veterinarian due to accidental injury, spontaneous bleeding, genetic screening, or blood tests. Pathogenesis Hemostasis is achieved through a series of events known as the coagulation cascade, which involves two interconnected pathways: the intrinsic and extrinsic pathways. The intrinsic pathway is triggered by spontaneous internal damage to the blood vessel lining, while the extrinsic pathway is activated in response to external trauma. Factor VII (FVII) is a vitamin K-dependent glycoprotein produced in the liver and released into the bloodstream as a single-chain zymogen. Once activated, FVII plays a crucial role in initiating coagulation. Following vascular injury, FVII, along with tissue factor (TF) and calcium, activates factors IX and X, leading to thrombin production. A deficiency in FVII impairs blood clotting, resulting in excessive bleeding during injuries or surgeries. Diagnosis The Buccal Mucosal Bleeding Time (BMBT) is the most commonly used test for measuring bleeding time in small animals. To perform the BMBT, the upper lip is folded back and secured with a gauze strip around the maxilla or both the maxilla and mandible. A small incision is made in the mucosa above the premolars, avoiding areas with visibly engorged vessels. Blood from the incision is gently blotted using filter paper placed near the incision without touching it. A stopwatch starts when the incision is made and stops when no blood crescent forms on the filter paper. To reduce variability, the same person should perform the BMBT whenever possible. Activated Partial Thromboplastin Time (APTT) measures the overall speed of blood clot formation through the intrinsic and common coagulation pathways. It assesses the activity of factors XII, XI, IX, VIII, X, V, II, I, as well as prekallikrein (PK) and high molecular weight kininogen (HK). Prothrombin Time (PT) is used to evaluate the extrinsic and common pathways of coagulation by measuring factors VII, X, V, II, and I. Factor VII deficiency is suspected when a dog presents with a prolonged PT and normal BMBT and APTT. Genetic testing can also identify affected dogs or carriers, especially in certain breeds. Breeds at Risk Canine Factor VII deficiency has been documented in several breeds, including the Beagle, Airedale, Alaskan Klee Kai, American Foxhound, Finnish Hound, German Wirehaired Pointer, Giant Schnauzer, Irish Water Spaniel, Japanese Spitz, Miniature Schnauzer, Papillon/Phalene, Sealyham Terrier, Scottish Deerhound, and Welsh Springer Spaniel. Management There is currently no cure for Factor VII deficiency. However, clinical symptoms can be managed through transfusions with fresh plasma or blood, or by administering recombinant activated human FVII. These treatments provide only temporary relief. Fortunately, dogs with mild to moderate FVII deficiency typically lead normal lives. References Callan MB, Aljamali MN, Margaritis P, Griot-Wenk ME, Pollak ES, Werner P, Giger U, High KA. A novel missense mutation responsible for factor VII deficiency in research Beagle colonies. J Thromb Haemost. 2006 Dec; 4(12):2616-22. Carlstrom LP, Jens JK, Dobyns ME, Passage M, Dickson PI, Ellinwood NM. Inadvertent propagation of factor VII deficiency in a canine mucopolysaccharidosis type I research breeding colony. Comp Med. 2009 Aug;59(4):378-82. Donner J, Kaukonen M, Anderson H, Moller F, Kyostila K, Sankari S, Hytonen M, Giger U, Lohi H. Genetic Panel Screening of Nearly 100 Mutations Reveals New Insights into the Breed Distribution of Risk Variants for Canine Hereditary Disorders. PLoS One. 2016 Aug 15;11(8):e0161005. Kaae JA, Callan MB, Brooks MB. Hereditary factor VII deficiency in the Alaskan Klee Kai dog. J Vet Intern Med. 2007 Sep-Oct;21(5):976-81.
Pyruvate Kinase Deficiency in Dogs

Bioguard Corporation Pyruvate kinase deficiency (PKD) is a hereditary genetic disorder that impairs the ability of red blood cells to metabolize properly. This defect leads to the destruction of red blood cells, resulting in severe hemolytic anemia. Affected animals can die from complications such as severe anemia and liver failure. The condition typically manifests between 4 months and 4 years of age, with common clinical signs including weakness, increased heart rate, and heart murmurs. Pathogenesis In mammals, mature red blood cells lack mitochondria, which means they cannot produce energy through oxidative phosphorylation. Instead, they rely on glycolysis to generate ATP, which is essential for maintaining cell shape and active transport across cell membranes. Pyruvate kinase (PK) plays a key role in the final step of glycolysis, where it catalyzes the conversion of phosphoenolpyruvate into pyruvate, producing ATP in the process (as shown in the diagram below). When PK is deficient, red blood cells cannot synthesize sufficient ATP, leading to impaired cell metabolism. This energy deficit causes premature red blood cell death and results in hemolytic anemia. PKD is an autosomal recessive disorder caused by mutations in the PK-LR gene, which affects the activity of pyruvate kinase. Clinical Symptoms Pyruvate kinase deficiency (PKD) typically presents between 4 months and 4 years of age, causing severe chronic hemolytic anemia. Affected dogs may display symptoms such as exercise intolerance, severe limb weakness, easy fatigue, lethargy, underweight, pale gums, weight loss, emaciation, stunted growth, poor posture, and an increased heart rate. Ultrasound exams may reveal an enlarged liver and spleen, with common findings like bone sclerosis and hemosiderosis/hemochromatosis. Treatment and Prevention Currently, there is no effective drug treatment or way to slow the progression of PKD. The only treatment option is bone marrow transplantation, which may allow dogs to live a normal lifespan. However, this treatment is costly and carries a risk of death. Without treatment, affected dogs typically succumb to severe hemolytic anemia and liver failure. Genetic testing can identify PKD defects early in dogs and cats, enabling timely intervention and care. Affected Breeds Research indicates that certain dog breeds are more predisposed to inheriting PKD, including: Basenjis, Labrador Retrievers, Pugs, West Highland White Terriers, Cairn Terriers, Dachshunds, Terriers, Miniature Poodles, Chihuahuas, and American Huskies. Among cat breeds, Somali and Abyssinian cats are commonly affected, along with Egyptian Maus, LaPerms, American Shorthairs, Bengals, Maine Coons, Norwegian Forest Cats, Siberians, and Singapuras. Genetic Detection Genetic testing can determine whether dogs and cats carry PKD defects. Carriers may pass the gene on to offspring, so they should not be bred. If an animal tests positive for PKD, early monitoring and care are essential to manage the disease. References Chapman, B.L., & Giger, U. (1990). Inherited erythrocyte pyruvate kinase deficiency in the West Highland White Terrier. Journal of Small Animal Practice, 31, 610-616. Schaer, M., Harvey, J.W., Calderwood-Mays, M., & Giger, U. (1992). Pyruvate kinase deficiency causing hemolytic anemia with secondary hemochromatosis in a Cairn Terrier. Journal of the American Animal Hospital Association, 28(3), 233-239. Gultekin, G.I., Raj, K., Foureman, P., Lehman, S., Manhart, K., Abdulmalik, O., & Giger, U. (2012). Erythrocytic pyruvate kinase mutations causing hemolytic anemia, osteosclerosis, and secondary hemochromatosis in dogs. Journal of Veterinary Internal Medicine, 26(4), 935-944.
Juvenile Hereditary Cataracts in Dogs
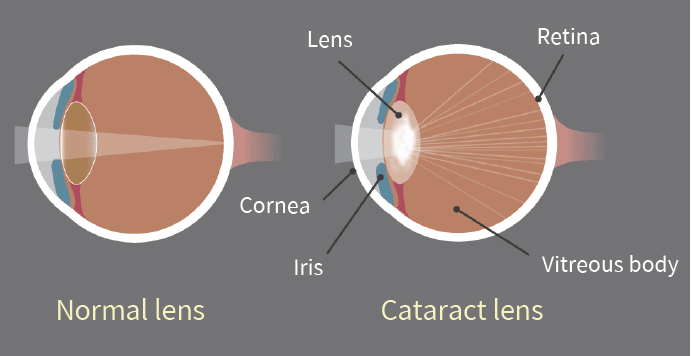
Bioguard Corporation Canine juvenile cataract (JHC) is a hereditary form of cataract characterized by cloudiness and degeneration of the lens in the eye. This condition prevents light and images from passing through the lens to the retina, impairing the dog’s vision and eventually leading to blindness. Affected dogs may exhibit symptoms such as bumping into furniture, losing direction, and moving slowly. JHC can also lead to intraocular complications, including uveitis, glaucoma, and lens luxation. Dogs are more prone to cataracts than any other species, and while cataracts can develop at any age, juvenile cataracts typically occur in dogs under 7 years old. Genetic mutaion related to JHC JHC is caused by a mutation in the heat shock transcription factor 4 (HSF4) gene, leading to an autosomal recessive inheritance pattern. Assuming that “A” represents a normal allele and “a” a mutated allele, an individual will exhibit symptoms of the disease only if both alleles are mutated (aa). Diagnosis A comprehensive ophthalmological examination is essential to assess the severity of cataracts and identify any associated complications. This examination typically includes tests for vision, pupillary light reflex, cataract severity and grading, and checks for any concurrent eye diseases or complications. Additional tests may include intraocular pressure measurement, tear production evaluation, corneal health assessment, fundus reflex and retinal examination, and ocular ultrasound. Genetic testing can further confirm the presence of genetic defects and is valuable as a pre-breeding health check to prevent the transmission of hereditary cataracts to offspring. Affected Breeds Breeds that are particularly prone to hereditary cataracts include Poodles, Cocker Spaniels, Boston Terriers, Siberian Huskies, Karelian Bears, Wire-haired Fox Terriers, Old English Sheepdogs, Golden Retrievers, and Labradors. It is recommended to conduct genetic testing before breeding these dogs to reduce the risk of producing affected offspring. Stages Cataracts can be classified into four stages based on the degree of lens opacity: Initial Stage: A distinct opaque white spot appears in the center of the pupil, but vision remains unaffected. Immature Stage: The lens begins to thicken both in the front and back, showing partial cloudiness. Vision becomes blurry, especially in low-light conditions, although some vision is still retained. Mature Stage: The entire lens becomes fully opaque and thickened, resulting in complete vision loss. Hypermature Stage: The clouded lens begins to shrink and clear up, making this stage prone to additional complications such as uveitis, glaucoma, and severe intraocular inflammation. This stage may also involve lens dislocation or fibrosis of the posterior capsule. Impacts and Complications The most noticeable early sign of cataracts is a change in eye color, where the lens begins to appear cloudy and white. It’s important to distinguish this from nuclear sclerosis, a common condition in older dogs. As the lens becomes cloudier, a dog’s vision deteriorates, leading to unintentional collisions with objects and increased sensitivity to the environment, often giving the dog a distant or blank stare. Cataracts typically worsen over time, resulting in a range of eye-related complications. These can include increased sensitivity, lens-induced uveitis (LIU), glaucoma, and the rupture of zonular fibers around the lens, which may cause lens dislocation or subluxation, as well as opacification of the posterior capsule. As cataracts progress to the hypermature stage, additional complications such as intraocular bleeding, retinal detachment, and further instances of glaucoma may arise. Early diagnosis and treatment are essential for managing these complications effectively and improving the overall prognosis. Diagnosis A comprehensive ophthalmological examination is essential to assess the severity of cataracts and identify any associated complications. This examination typically includes tests for vision, pupillary light reflex, cataract severity and grading, and checks for any concurrent eye diseases or complications. Additional tests may include intraocular pressure measurement, tear production evaluation, corneal health assessment, fundus reflex and retinal examination, and ocular ultrasound. Genetic testing can further confirm the presence of genetic defects and is valuable as a pre-breeding health check to prevent the transmission of hereditary cataracts to offspring. References Mellersh CS, McLaughlin B, Ahonen S, Pettitt L, Lohi H, Barnett KC. Mutation in HSF4 is associated with hereditary cataract in the Australian Shepherd. Vet Ophthalmol. 2009 Nov-Dec; 12(6):372-8. Mellersh CS, Pettitt L, Forman OP, Vaudin M, Barnett KC. Identification of mutations in HSF4 in dogs of three different breeds with hereditary cataracts. Vet Ophthalmol. 2006 Sep-Oct; 9(5):369-78.
Spinal Muscular Atrophy in Cats

Bioguard Corporation Spinal muscular atrophy (SMA) an autosomally recessive inherited neurodegenerative disorder seen in Maine Coon cats. The disease is characterized by weakness and atrophy in muscles due to loss of motor neurons that control muscle movement. Affected cats first show signs of disease around 3–4 months of age. Clinical signs include tremors, abnormal posture, and weakness in muscle. Pathogenesis SMA in Maine Coon cat is caused by the deletion of a 140 kb LIX1 gene on the A1q chromosome. Although the function of LIX1 is not yet clear, it is presumed to be related to RNA metabolism. The LIX1 is highly expressed in the central nervous system, primarily in spinal motor neurons, thus offering explanation of the restriction of their function in case of feline SMA. The disease is inherited as an autosomal recessive. Clinical signs In the earliest stages of SMA, a vet or other professional will be able to notice a slight weakness in the affected kittens. Subtle tremors in a kitten’s hind legs can also be an early symptom of SMA. Within 1 to 2 months after the symptoms appear, the muscles will gradually atrophy. After that, the symptoms will gradually become serious, the movements will become clumsy, the agility will be lost in jumping, and even breathing symptoms will appear. Muscle atrophy affects only the hind legs, and some severely affected cats move by crawling on the front legs, although mental status is not affected. The condition slowly stabilizes after up to 8 months, and some cats with SMA have more or less severe symptoms for up to 9 years. Diagnosis The first step is a general physical exam. Your doctor will look for muscle weakness and any other signs of SMA. Serum creatine kinase (creatine) elevations and electrical findings in cats are very similar to mild spinal muscular atrophy in humans. Examination of the muscles reveals neurogenic atrophy, and examination of the central and peripheral nervous systems will reveal loss of anterior horn cells. To ascertain if a cat has SMA, the diagnostic approach encompasses a physical examination, electromyography, muscle biopsy, testing for serum creatine kinase levels, and genetic testing, all aimed at facilitating early identification and intervention. Since SMA is common in Maine Coons, it is recommended that Maine Coons with similar symptoms or those intended for breeding undergo this test. References Fyfe JC, Menotti-Raymond M, David VA, et al. An approximately 140-kb deletion associated with feline spinal muscular atrophy implies an essential LIX1 function for motor neuron survival. Genome Res. 2006 Sep;16(9):1084-90.
Polycystic Kidney Disease in Cats

Bioguard Corporation Polycystic kidney disease (PKD) is a chromosomally dominant genetic disorder; it can occur in humans, cats, dogs, and other animals. In the renal cortex and medulla, there are cysts of various sizes and fluid-filled, so it is commonly known as the bubble kidney. Cysts increase in size and number over time, replacing kidney tissue and affecting their ability to filter waste from the blood, leading to chronic kidney failure. Pathogenesis Polycystic kidney disease is primarily caused by point mutations in the PKD1 gene, which is inherited as a dominant genetic disorder. The PKD1 gene plays a crucial role in regulating polycystin, a protein found on the cell membrane. A deficiency in PKD1 leads to underdevelopment of the renal tubules and collecting ducts in the renal cortex and medulla, preventing proper drainage of urine filtered by the renal glomeruli, which results in the formation of cysts characteristic of polycystic kidney disease. In the liver, this condition can also cause significant enlargement of bile ducts near the portal vein and may lead to bile duct fibrosis. Clinical symptoms Cats with polycystic kidney disease (PKD) are born with abnormal kidneys, though symptoms typically do not manifest until they are between 3 and 10 years old, with an average onset around 7 years. While the disease is present from birth, there are no noticeable symptoms in its early stages. Symptoms appear only when the disease progresses to a point where kidney tissue necrosis and kidney failure occur. As renal cysts enlarge over time, they compress the renal parenchyma, leading to irreversible kidney failure. Affected cats may experience a decreased appetite, weight loss, depression, and lack of energy. Clinical symptoms include increased thirst (polydipsia), frequent urination (polyuria), anorexia, vomiting, lethargy, and muscle twitching in the abdominal area. In severe cases, movement disorders (ataxia) or neurological issues may arise. Blood tests may reveal elevated blood urea nitrogen (BUN) and creatinine (CRE) levels, anemia, and high blood pressure. Early detection At present, it is possible to know whether cats have polycystic kidney disease through ultrasound testing and genetic testing. At 16 weeks of age, about 75% of cats with this problem had cyst-like structures on ultrasound scans, and by 36 weeks of age, 91% of cats had cysts. The accuracy of such a structure increases with age; generally speaking, when cats are over 10 weeks old, when using ultrasonic scanning, the accuracy can reach 90~95%. Genetic testing, which refers to the detection of its genotype, will be 100% accurate and can be performed at any age Breed predisposition Polycystic kidney disease mainly occurs in long-haired cats, and studies have shown that up to 38% of Persian cats have an abnormal PKD1 gene. Mainly affects cats of Persian and Persian-related breeds, such as Chinchillas, but other breeds such as Ragdolls, Scottish Folds, or other shorthair breeds such as Himalayans and Exotics have also been reported It is possible to have this genetic disorder. In addition, Meeks’s condition is relatively rare. References Schirrer L, Marín-García PJ, Llobat L. Feline Polycystic Kidney Disease: An Update. Vet Sci. 2021 Nov 8;8(11):269.