
Breed-related disease: Sphynx cat

The Sphynx cat is a breed of cat known for its lack of coat (fur). Hairlessness in cats is a naturally occurring genetic mutation; however, the Sphynx cat, as a breed, was developed through selective breeding. The Sphynx first appeared as a natural mutation in Canada in 1966. The first hairless male, Prune, was mated back to his mother, and some of their hairless kittens were exported to Europe, where they acquired the breed’s name. Despite appearances they’re not completely naked and their skin has the texture of a peach – Sphynx should not be described as bald! They’re warm to the touch too! It really is difficult to judge or appreciate Sphynx just from photographs. What wins people over, beyond the appeal of the unusual, is their larger-than-life characters. It is possibly one of the most affectionate, sociable and intelligent cats in the world, they adore human attention and enjoy cuddles and games. They are outgoing, mischievous, people-orientated and loves attention. These cats often greet their owners when they come home and are very talkative. They are highly intelligent, playful and cuddly. They like to sleep with their owners – under the covers. Their body temperature is a degree or two above the average for normal cats and they have voracious appetites to compensate for the heat loss. With little protection against the elements, these cats cannot be left out in the cold, they don’t like to sit on cold surfaces and they do appreciate central heating! Those that do go outside in the sun may need sun protection on pale skin. We know that because you care so much about your cat, you want to take great care of her. That is why we have summarized the health concerns we will be discussing with you over the life of your Sphynx. By knowing about the health concerns common among Sphynxes, we can help you tailor an individual preventive health plan and hopefully prevent some predictable risks in your pet. Heart Disease: the sphinx is prone to cardiomyopathy which is the medical term for heart muscle disease, either a primary inherited condition or secondary to other diseases that damage the heart. The most common form, called hypertrophic cardiomyopathy, or HCM, is a thickening of the heart muscle often caused by an overactive thyroid gland. Blood Type: Just like people, individual cats have different blood types. Most domestic cats have type A blood, but purebred cats, like your Sphynx often have a different blood type, usually type B or very rarely, type AB. Determining your cat’s blood type is essential before starting a transfusion, so knowing your cat’s type ahead of time can save crucial minutes. For more information regarding the blood typing please visit following link: https://www.bioguard.com.tw/en/project/feline-blood-typing-kit/ Alopecia: If you thought you were getting out of grooming chores by adopting a Sphynx cat, think again! Your sphynx Cat’s skin will build up a greasy grunge if left unbathed—and don’t forget the ears! The insides of the ears will get waxy and need to be cleaned periodically as well. Urticaria Pigmentosa: There is a long list of diseases that can make your cat itch and break out in little red bumps. Allergies to food or to pollen, parasites like fleas or mites, fungal or bacterial infections, and even certain types of autoimmune diseases can all cause these general symptoms. But for your Sphynx, add urticaria pigmentosa to the list. The exact pathology of this itchy skin disease has not yet been fully discovered, but it appears to be passed on genetically, and is fairly common in some family bloodlines. With so many possibilities as the cause for apparently identical skin irritations, diagnostic testing is essential in order to narrow down treatment options. Sources: https://www.yourcat.co.uk/types-of-cats/sphynx-cat-breed-information/ https://chesapeakevetclinic.com/client-resources/breed-info/sphynx/ photo credit: https://www.freepik.com/premium-photo/hairless-canadian-sphynx-cat-with-bow-tie-isolated_6884985.htm
Case study: Cerebral toxoplasmosis in a cat with feline leukemia and feline infectious peritonitis viral infections
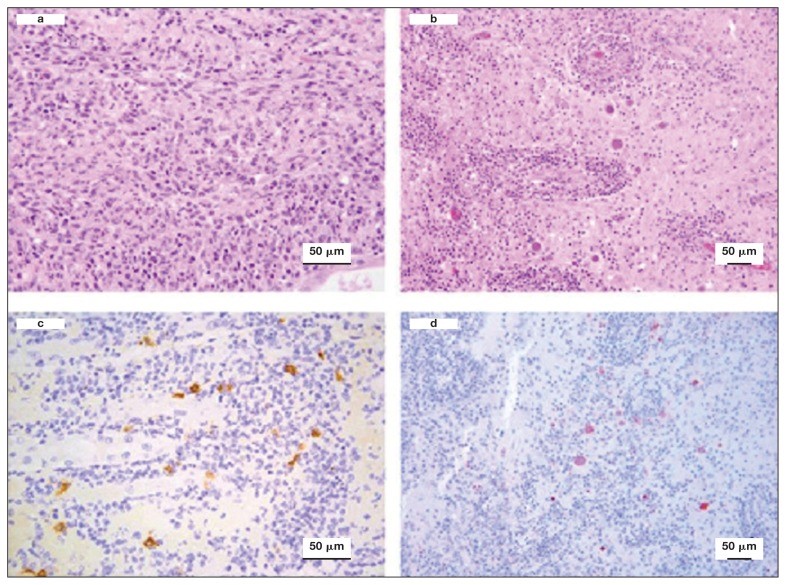
Case study: Cerebral toxoplasmosis in a cat with feline leukemia and feline infectious peritonitis viral infections Robert Lo, Ph.D, D.V.M A diarrheic young cat died because of severe multifocal meningoencephalitis caused by Toxoplasma gondii. Protozoan cysts and tachyzoites in the brain were confirmed by immunohistochemical staining. Coinfection of feline leukemia virus (FeLV) and feline infectious peritonitis (FIP) might be the possible contributors to the clinical, fatal outcome. Original paper: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6049326/ Histological lesions and immunohistochemistry (IHC) of the brain and kidney of a 6-month-old cat that was diagnosed with cerebral toxoplasmosis following postmortem examination. a — Kidney showing chronic pyogranulomatous nephritis. Hematoxylin and eosin (H&E), 40×. b — Brain showing perivascular cuffing of lymphocytes and plasma cells with multifocal vasculitis. Many oval protozoan cysts having a thin wall and containing basophilic bradyzoites were seen near to the vascular structures. H&E, 20×. c — Kidney stained by IHC with feline coronavirus antibodies showing multifocal positive reaction in the cytoplasm of macrophages, 40×. d — Brain stained by IHC with anti-Toxoplasma gondii antibodies and showing several positively stained protozoan cysts and tachyzoites, 20×.
The Shiba Inu

John K. Rosembert The Shiba Inu dog breed was originally bred to flush birds and small game and was occasionally used to hunt wild boar. It is the smallest of the six original and distinct spitz breeds of dog native to Japan. the Shiba Inu dog almost died out entirely in the Second World War but the small number of dogs who had survived bombing raids and a distemper epidemic were bred to save the breed. It is a small, compact dog, their head is in proportion with the body with a round muzzle that has a moderate stop and tapers slightly toward the nose. The tight lips and the nose are black. The teeth meet in a scissors bite. The deep-set eyes are triangular in shape and dark in color. The well-bred Shiba Inu is good-natured, alert, and bold. He is strong-willed and confident and often has his own ideas about things. He is loyal and affectionate with his family, though tends to be suspicious of strangers. The Shiba Inu doesn’t share well. He tends to guard, sometimes aggressively, his food, toys, or territory. And he doesn’t always get along with other dogs, especially if he’s intact. He won’t hesitate to chase small animals that he considers prey. This is a smart breed, but training a Shiba Inu isn’t like training a Golden Retriever. While a Golden is delighted to come when called, the Shiba Inu will come when he feels like it — or not. He’s been described as stubborn, but freethinking is probably a more positive way to characterize him. Below we will discuss the most common health problems that Shiba Inu may encounter during his lifetime. Eye Problems: Not many things have as dramatic an impact on your dog’s quality of life as the proper functioning of his eyes. Unfortunately, Shiba Inus can inherit or develop several different eye conditions, some of which may cause blindness if not treated right away, and most of which can be extremely painful! We will evaluate his eyes at every examination to look for any signs of concern. Ex: Glaucoma, Cataracts, Distichiasis, Eyeballs. Pyometra: If a female Shiba Inu hasn’t been spayed, then they can experience pyometra during their heat cycle. It occurs when the growth of cells in the uterus is at its highest production rate (this happens during their heat cycle), in which bacteria can migrate into the area and cause a life-threatening infection. While this condition can occur to all-female canines, it seems to be a bit more prominent with Shibas, which only furthers the reason they should be spayed. Heart Disease: Some breeds like your Shiba can be born with a variety of heart defects. Most of these affect the structure of the heart’s dividing wall or the vessels. They can also cause problems with the electrical signals that control the heartbeat or with heart valve function. Allergies: In humans, an allergy to pollen, mold, or dust makes people sneeze and their eyes itch. In dogs, rather than sneeze, allergies make their skin itchy. We call this skin allergy “atopy”, and Shibas often have it. Commonly, the feet, belly, folds of the skin, and ears are most affected. Symptoms typically start between the ages of one and three and can get worse every year. Licking the paws, rubbing the face, and frequent ear infections are the most common signs. The good news is that there are many treatment options available for this condition. Seizures: Seizures in dogs aren’t exactly similar to what humans are used to. They can take shape as the Shiba Inu running around ceaselessly, hiding in corners in complete confusion, barking at nothing, and freezing up. While seizures are usually not life -threatening for dogs, they can also be indicative of a more serious problem. https://dogtime.com/dog-breeds/shiba-inu#/slide/1 https://animalhealthcenternh.com/client-resources/breed-info/shiba-inu/ https://canna-pet.com/shiba-inu-health-problems-issues/ Photo credit: https://thehappypuppysite.com/shiba-inu-temperament/ https://en.wikipedia.org/wiki/Shiba_Inu
Breed-related disease: Scottish Fold

John K. Rosembert The Scottish Fold is a medium-size cat with a rounded head and big round eyes, although he is known for his standout feature: ears that fold forward, giving him the appearance of a furry owl. His coat, which comes in many colors and patterns, can be short or long. The long-haired variety is known as the Highland Fold. Drop-eared cats such as the Scottish Fold are not as unusual as they might seem. Spontaneous genetic mutations, such as curly coats or folded ears, occur in cats on a fairly regular basis, and the Scottish Fold is the result of such a mutation. All of today’s Folds descend from a Scottish fold-eared cat named Susie who was found by a shepherd in 1961. Scottish Fold kittens are born with what look like normal ears. The ears soon begin to bend forward, usually two to four weeks after birth. By the time he is three months old, the typical Scottish Fold has a distinctly owlish look, the tightly folded ears do not appear to be any more prone to infections than those of cats with upright ears. However, this unique ear shape is caused by an underlying defect in the formation of cartilage, which would normally retain the ears in a normal shape. This inherited cartilage defect (also known as Scottish Fold disease, or Osteochondrodysplasia) causes other deformities throughout the body and is a dominant trait, meaning all kittens in the litter will be affected. The disease is evident on x-rays of cats from as young as 7 weeks of age. Serious abnormalities in joints and bone growth lead to arthritis (painful, swollen joints), short, abnormally thick and inflexible tails, spinal abnormalities and short, stiff legs. The welfare impacts are severe in terms of pain and inability to perform natural behaviors, as these cats can be lame, walk with an abnormal gait, can be reluctant to engage in normal movements such as walking or jumping, and can even become completely crippled. That’s why breeding the Scottish Fold is banned in some country. The Scottish Fold is a great family pet. They are very loyal to their family. They are not a shy breed that would hide around the house; they prefer always being around and following owners from room to room. Scottish Folds are very intelligent and inquisitive. They learn to open cabinets, play fetch, sit up, and some like to eat & drink with their paws. Most love to drink from running water! Most Scottish Folds also “sit up” like a prairie dog when they hear something to get a look around. Below we summarized some of the most common health issues of Scottish Fold cat in order to help you prevent some predictable risks in your pet. Dental disease is one of the most common chronic problems in pets who don’t have their teeth brushed regularly. Unfortunately, most cats don’t take very good care of their own teeth, and this probably includes your Fold. Polycystic kidney disease (PKD) is caused by a defective gene. The disease was first recognized in Persians, and is seen occasionally in other breeds, including Shorthaired Scottish Folds. Affected kittens are born with miniscule cysts inside the kidneys and sometimes the liver that slowly enlarge over time, eventually destroying the affected organ. FLUTD Feline lower urinary tract disease (FLUTD) is not a specific disease, but rather is the term used to describe conditions that can affect the urinary bladder and/or urethra (the lower urinary tract) of cats. This situation is very common in Scottish Fold. Sources https://canalclinic.com/client-resources/breed-info/scottish-fold-shorthair/ Photo credit https://scottishfoldcats.net/scottish-fold-munchkin-cat-price/ https://commons.wikimedia.org/wiki/File:Scottish_fold_cat.jpg
The Feline Herpesvirus: An Overview
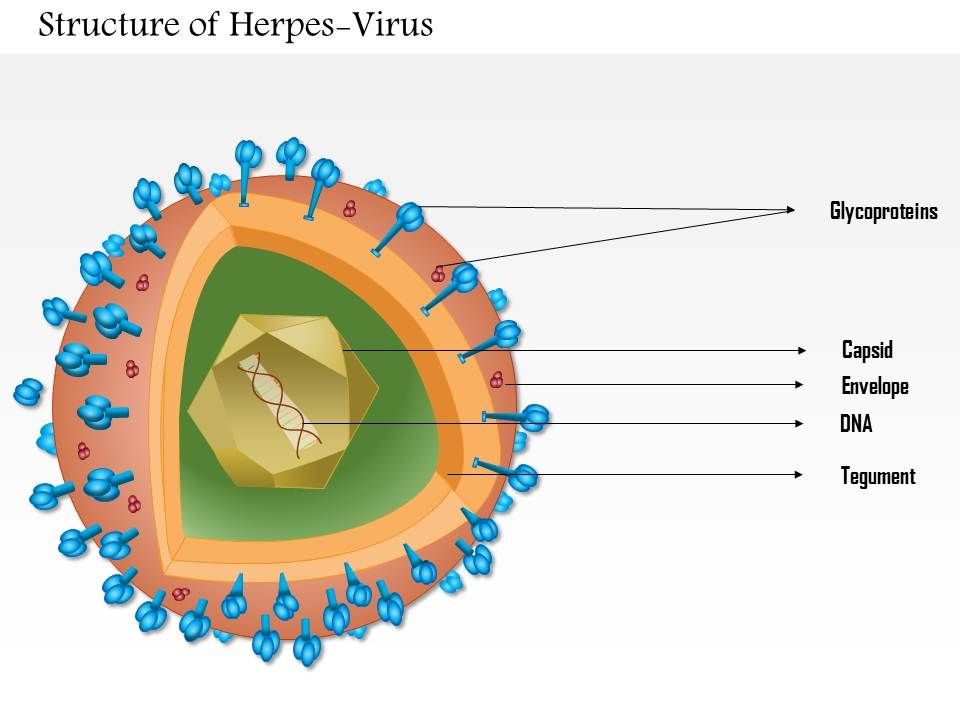
The Feline Herpesvirus: An Overview Maigan Espinili Maruquin The feline herpesvirus infection is common and recurring ocular disease is common (Stiles 2000). It is the most studied infectious cause of ocular surface disease in cats (Andrew 2001). Developing latent infections may recrudesce at later points in life of an infected cat (Stiles 2000). I. Structure and Replication Fig. 01. Structure of Herpes Virus. https://www.slideteam.net/0814-herpes-virus-medical-images-for-powerpoint.html The feline herpesvirus (FHV 1) causes feline viral rhinotracheitis (FVR) (Gaskell and Wardley 1978, Gaskell, Dawson et al. 2007, Henzel, Brum et al. 2012). This virus is double-stranded DNA with a glycoprotein-lipid envelope and is a member of the Varicellovirus genus in the Alphaherpesvirinae subfamily (Gaskell, Dawson et al. 2007). This virus was also found out to be relatively fragile in the external environment and is highly susceptible to the effects of common disinfectants (Scott 1980, Eleraky, Potgieter et al. 2002, Gaskell, Dawson et al. 2007). The FHV- 1 has short replication cycle, rapid cell-to-cell spread, has tendency to induce cell lysis, and displays persistence in sensory ganglia of their host (Gould 2011). It replicates in epithelial cells of both the conjunctiva and upper respiratory tract, and in neurons. The neuronal infection can lead to a lifelong latency after the primary infection (Thiry, Addie et al. 2009). For 18 hours, it can survive in damp environment, less in dry conditions and is also recorded to be relatively unstable as an aerosol (Povey and Johnson 1970, Donaldson and Ferris 1976, Stiles 2000, Gaskell, Dawson et al. 2007, Gould 2011). II. Infection and Epidemiology There are only three main genotype groups recognized for FHV-1 strains with very little genomic variations (Gould 2011). The virus sheds in ocular, nasal, and oral secretions with large transmission by direct contact with an infected cat. Although one of the most important sources of virus are the acutely infected cats, susceptible cats may also be infected by latently infected carrier cats (Gaskell and Povey 1982, Gaskell, Dawson et al. 2007). On the other hand, the environment may not be a primary source of transmission but catteries may cause indirect transmission through contaminated housing, feeding and cleaning utensils, and personnel (Gaskell, Dawson et al. 2007, Thiry, Addie et al. 2009). Latently infected cats may also transmit FHV to their kittens due to the parturition and lactation inducing stress that may lead to viral reactivation and shedding, making kittens susceptible to the virus, depending on the level of maternally derived antibodies (MDA) they possess. High levels of MDA protects kittens against the disease and may develop subclinical infection leading to latency while insufficient MDA may lead to clinical signs (Gaskell and Povey 1982, Thiry, Addie et al. 2009). Recovered cats become latently infected carriers and reactivation happens particularly after periods of stress (Gaskell, Dawson et al. 2007). However, it doesn’t shed immediately after the stress. It undergoes lag phase of 4–11 days, precedes the shedding from 1–13 days (Gaskell and Povey 1973, Gaskell and Povey 1977, Gaskell, Dawson et al. 2007). Further, risk factors associated with FeHV-1 shedding includes contact with other cats, the presence of upper respiratory disease, younger cats, poor hygiene, and larger households (Sykes, Anderson et al. 1999, Binns, Dawson et al. 2000, Helps, Lait et al. 2005, Gaskell, Dawson et al. 2007). III. Pathogenesis Infection routes include nasal, oral, and conjunctival mucous membranes and is primarily shed in secretions for 1–3 weeks following infection (Andrew 2001, Gaskell, Dawson et al. 2007). In pregnant queens, vaginitis was caused by intravaginal instillation virus and causes congenitally infected kittens while intravenous inoculation leads to transplacental infection and abortion (Bittle and Peckham 1971, Hoover and Griesemer 1971, Gaskell, Dawson et al. 2007). After 1 to 2 exposure of naive animals to FHV-1, the viral replication happens and epithelial cell necrosis occur in the nasal turbinates, nasopharynx and conjunctival mucosa (Gaskell & Dawson 1998). Lytic infection of the nasal epithelium with spread to the conjunctivas, pharynx, trachea, bronchi and bronchioles occurs and lesions characterized by multifocal epithelial necrosis with neutrophil infiltration and inflammation are also observed. Moreover, neonates or hypothermic kittens display transient viraemia associated with mononuclear cells (Gaskell, Dawson et al. 2007, Thiry, Addie et al. 2009). It has been recorded that almost all infected cats become lifelong carriers. During the latency period, virus was spread along the sensory nerves and neurons with viral genome doesn’t replicate. Whereas, reactivating stressors include lactation and moving into a new environment (Gaskell and Povey 1977, Gaskell and Povey 1982, Pedersen, Sato et al. 2004, Thiry, Addie et al. 2009). Lesions may be developed upon viral reactivation in adult cats and ‘recrudescence’ disease may also be a consequence (Thiry, Addie et al. 2009). As high as 70% mortality rates was reported for infected kittens (Povey 1990). Although MDA may persist for 2 to 10 weeks, this may not protect cats from subclinical infection (Gaskell & Dawson 1998)(Andrew 2001). IV. Clinical Signs Generally, FHV- infected cats display acute upper respiratory and ocular disease with usually 2 to 6 days incubation period, or may be longer (Gaskell and Povey 1979, Stiles 2000, Gaskell, Dawson et al. 2007) with depression, fever, lethargy, inappetence, pyrexia, sneezing, coughing, nasal discharge, and conjunctivitis with ocular discharge depending on the viral exposure and individual susceptibility (Hoover, Rohovsky et al. 1970, Crandell 1973, Stiles 2000, Gaskell, Dawson et al. 2007, Thiry, Addie et al. 2009) (Gaskell R.M., Dawson S, 1994). Also, excessive salivation with drooling may also be observed during the initial clinical signs of the disease (Gaskell, Dawson et al. 2007).Once the virus reaches the lungs, pneumonia may kill the infected kittens (Stiles 2000, Thiry, Addie et al. 2009) (Gaskell R, et al. 2006). The primary FHV- 1 infection with secondary bacterial infection leads in conjunctivitis sometimes with severe hyperemia and chemosis. The conjunctivitis is manifested as hyperaemia or redness with serous discharge, progressing to mucopurulent ocular discharge whereas, chemosis is swelling or oedema of the conjunctiva which may occur to
Symmetric dimethylarginine (SDMA)
Symmetric dimethylarginine (SDMA) Andy Pachikerl, Ph.D Introduction For over a millennium and a few centuries, urinalysis has given leads to medical diagnoses. It was until the repetitive use of clinical chemistry approximately 50 – 60 years that these data of renal biomarkers became commonplace in human and veterinary medicine. From here onwards, both an improved understanding of the renal system and ability to diagnose renal disease was updated. In the past, renal biomarkers have focused on kidney function testing, and this is the basis for current conventional test in blood (serum creatine [sCr], urea or urea nitrogen [UN] as endogenous indicators of glomerular filtration rate [GFR]). Recently, we are becoming more aware of the need to identify renal disease at an early stage when therapeutic options are most effective. Both sCr and UN both play vital role in diagnosis of kidney disease, their limitations create poor confidence for their use as early indicators for disease. New markers of renal function try to overcome these limitations. Additionally, there are now many urinary markers that can detect kidney damage and help localize that damage to the compartment of the kidney that is affected. Endogenous markers of GFR Creatine The most common endogenous marker for estimating GFR is serum creatinine and its metabolism. Measurement and diagnostic significance in dogs have previously been reviewed (Braun, et al., 2003). Recent reviews, however, suggested factors that can either enhance or limit the clinical use of sCr to optimize diagnostician and clinical pathologist to interpret the data of this conventional test. Particularly, accurate interpretation of published data, population-specific reference intervals, trending of sCr and consideration of muscle mass influence and analytic variability are all needed to best interpret sCr in dogs and cats. Of note, although creatinine is referred to as sCr throughout this manuscript, creatinine is also commonly measured in plasma. Nephron mass vs nephron function. It is generally accepted that 75% of nephron mass must be lost before sCr increases above the reference limit (Braun, et al., 2003). The original source for this statement likely originates from partial nephrectomy studies in dogs. However, it is often mistaken for 75% loss of renal function vs mass. In partial nephrectomy studies, ¾ loss of renal mass related to about 50–60% or 35–45% reduction in renal function based on inulin clearance one month or 13 months post-surgery, respectively (Brown, et al., 1990; Bovee, et al., 1979). The much lower decrease in function as compared with the percentage of nephron loss is due to compensatory changes in remaining nephrons (ie, compensatory renal hypertrophy) (Brown, et al., 1990; Bricker, et al., 1964). Furthermore, using an age- and breed-specific reference limit (sCr ≥ 106 mmol/L or 1.2 mg/dL) along with frequent monitoring, adolescent dogs with rapidly progressive kidney disease due to X-linked hereditary nephropathy (XLHN) demonstrated increased sCr after GFR had decreased an average of 48% (range 39–68%).8 Based on these studies, sCr can be more sensitive for detecting decreased renal function than has been historically assumed. Value of population-specific reference intervals. While sCr is not as poorly sensitive as generally believed, its inability to regularly detect < 50% decline in kidney function at least partly stems from reference intervals that are overly wide for patients with low baseline sCr. Since current methodologies are highly specific for creatinine, the wide reference intervals largely stem from biologic differences in sCr among individuals. Serum creatinine has relatively high individuality in dogs and cats (Baral, et al., 2014; Ruaux, et al., 2011), meaning that variability between individuals is much higher than the variability observed within a single animal. Serum creatinine is influenced by age (Rosset, et al., 2012; Rørtveit, et al., 2015) and particularly by breed in dogs (Misbach, et al., 2014; Zaldívar-López, et al., 2011) and, to a lesser extent, in cats.20 It might also be influenced by sex and the veterinary clinic evaluating the patient.21 Therefore, sCr would benefit from age- and breed-specific reference intervals, ideally (although not practically) for every individual instrument and laboratory. Trending of serum creatinine. Small increases in sCr even within the reference interval can reflect significant decreases in GFR in an individual patient8, particularly since variation in sCr within an individual healthy dog or cat is minimal over weeks to months and even years (Braun, et al., 2003; Baral, et al., 2014; Ruaux, et al., 2011). In fact, the critical difference or reference change value for detecting a significant increase or decrease in sCr is only 23–27 lM/L (0.3 mg/dL) in clinically healthy dogs10, and 17% (corresponding to similar absolute values as in dogs) in clinically healthy cats (Braun, et al., 2003). Thus, the sensitivity of sCr for detecting early kidney disease can be improved by evaluating serial fasted sCr measurements in an individual animal (trending) to look for increases that likely reflect worsening renal function. This concept of detecting small but clinically relevant increases in sCr is actively being adopted in cases of acute kidney injury (AKI), illustrated by the International Renal Interest Society (IRIS) Grading of AKI. In this grading scheme, an increase in sCr ≥ 26 lmol/L (0.3 mg/dL) within a 48- hour period is a criterion for identifying Grade I and Grade II AKI (www.IRIS-Kidney.com). Furthermore, in adolescent dogs with XLHN, trending of sCr detected an average of 27% (range 5–49%) decrease in GFR (Nabity, et al., 2015). Despite heightened awareness of small, but clinically relevant increases in sCr over a short time frame, more recognition is needed with slowly progressive CKD, in which small increases might occur over many months or years. Analytic challenges. Finally, sCr is plagued by inconsistencies in its measurement between instruments and laboratories, which can result in markedly different results. While most reference laboratory instruments have excellent precision and provide results of similar magnitude among instruments (Ulleberg, et al., 2011), recent studies illustrate the high imprecision and bias possible with some instruments and among different laboratories (Ulleberg, et al., 2011; Braun, et al., 2008). In normal to mildly azotaemia samples,
Case study: Report of the first clinical case of intestinal trichomoniasis caused by Tritrichomonas foetus in a cat with chronic diarrhoea in Brazil
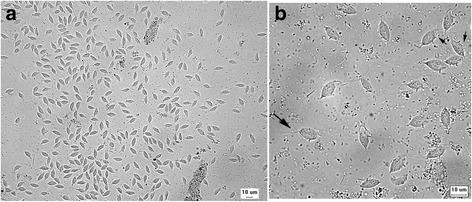
Case study: Report of the first clinical case of intestinal trichomoniasis caused by Tritrichomonas foetus in a cat with chronic diarrhoea in Brazil Robert Lo, Ph.D, D.V.M A seven-month-old, entire male domestic shorthair kitten was presented to the Veterinary Hospital of the School of Veterinary Medicine – University of São Paulo, Brazil. The cat showed a six-month history of persistent large intestinal diarrhoea, faecal incontinence, prostration, apathy and weight loss. P Protozoan parasites were observed under microscope using fresh fecal sample obtained via colon flush. Infection of Tritrichomonas foetus was confirmed by PCR and DNA sequencing. After treatment with ronidazole (30 mg/kg, PO q24h for 14 days), the cat showed resolution of clinical signs. This is the first clinical case of T. foetus infection in a chronic diarrheic cat in Brazil and South America. Original paper: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5392982/ Fig. 1 Tritrichomonas foetus in cat feces. a Numerous pyriform trophozoites. b The three free anterior flagella (large arrow) and the undulating membrane (small arrows) can be visualised in some trophozoites. Fresh preparation in saline 0.85%.
Beagle Breed Health Risks and Modern Diagnostic Approaches

Table of Contents 1. Introduction: The Beagle as a Functional Scent Hound The Beagle is a small hound breed developed primarily for hunting hare, distinguished by its exceptional sense of smell and persistent tracking ability. Closely resembling a smaller version of the foxhound, the Beagle has historically functioned as a scent-driven working dog, capable of following trails over long distances with remarkable accuracy. This olfactory specialization has extended beyond hunting; today, Beagles are widely used as detection dogs for prohibited agricultural products and food items in quarantine systems worldwide, reflecting the precision of their scenting capability. From a morphological standpoint, Beagles are compact yet robust, with a deep chest, strong limbs, and a short, dense coat—features that support endurance rather than speed. Their long head, low-set drooping ears, and expressive eyes are characteristic of scent hounds, while their sociable and gentle temperament has made them one of the most popular companion breeds globally. However, alongside these desirable traits, the breed is associated with a range of Beagle health problems that reflect both its genetic background and functional design. These include neurological disorders such as epilepsy, endocrine conditions like hyperadrenocorticism, and structural issues affecting the spine, eyes, and cardiovascular system. As veterinary medicine increasingly adopts precision and preventive approaches, understanding how these risks arise—and how they can be managed—is essential for improving long-term health outcomes in the breed. 2. Breed Morphology and Behavioral Characteristics The Beagle’s morphology and behavior are tightly linked to its historical role as an endurance scent hound, bred to track prey over long distances in challenging terrain. As with many working breeds, these functional traits confer both performance advantages and predictable clinical risks. 2.1 Morphology The physical build of the Beagle reflects its specialization for sustained scent tracking rather than speed, with anatomical features optimized for endurance, environmental resilience, and olfactory efficiency. 2.1.1 Coat and Coloration Beagles possess a short, dense, and weather-resistant “hound coat”, designed to protect against environmental exposure such as moisture and dense vegetation. Most commonly tricolor (black, white, and tan) Other variations include lemon and white or red and white Characteristic white-tipped tail (“flag”) enhances visibility in tall grass 2.1.2 Body Structure and Build Beagles are compact, sturdy, and slightly longer than tall, with a structure that supports endurance tracking: Deep, broad chest → increased lung capacity Strong, muscular back → sustained locomotion Short, stocky limbs → stability over uneven terrain This conformation allows Beagles to maintain prolonged activity at moderate intensity, a key trait for scent hounds. 2.1.3 Head and Expression The Beagle’s head is a functional sensory unit: Moderately long skull with slight dome Square-cut muzzle for efficient airflow Large brown or hazel eyes, producing the breed’s characteristic gentle expression Low-set, drooping ears, aiding in scent tracking 2.1.4 Clinical Risks Associated with Morphology While functionally advantageous, these traits contribute to specific health risks: Ear infections (otitis externa):Drooping ears restrict airflow, creating a warm, humid environment favorable for bacterial and yeast overgrowth Spinal disorders (IVDD):A relatively elongated back combined with compact limb structure can increase mechanical stress on intervertebral discs Clinical Insight:Even moderate conformation traits, as seen in Beagles, can produce measurable disease risk when combined with lifestyle and environmental factors. 2.2 Behavioral Characteristics The Beagle’s temperament reflects its development as a pack-oriented, scent-driven working dog, resulting in a unique combination of sociability, independence, and strong instinctual behavior. 2.2.1 Sociability and Temperament Beagles are widely regarded as: Friendly, gentle, and even-tempered Highly sociable with other dogs Particularly well-suited for families with children Their pack-based origin contributes to their strong social bonding behavior. 2.2.2 Separation Anxiety A direct consequence of their pack nature is a low tolerance for isolation: Prone to separation anxiety May exhibit destructive behaviors when bored or left alone Clinical Relevance:Chronic stress can contribute to behavioral disorders and secondary health issues. 2.2.3 Instinctual Drives and Roaming Behavior Beagles possess an exceptionally strong prey drive and scent-tracking instinct: Easily distracted by environmental scents May ignore recall commands once engaged in tracking Require secure fencing and leash control Behavioral Note:Early socialization is essential if cohabiting with non-canine pets. 2.2.4 Training and Cognitive Profile Although intelligent, Beagles exhibit: Independent, scent-driven decision-making Reduced responsiveness to repetitive obedience training Effective Training Strategy: Positive reinforcement Short, engaging sessions Use of food-based motivation 2.2.5 Vocalization (Baying) Beagles are known for their distinctive “baying” vocalization: A deep, resonant sound combining elements of a howl and bark Historically used to signal location during hunts Modern Context:This trait persists and can be a challenge in domestic environments. 2.2.6 Appetite and Obesity Risk Beagles have a markedly high appetite and food motivation, which presents both advantages and risks: Facilitates training Predisposes to: Overeating Ingestion of non-food items Clinical Impact of Obesity: Increased risk of: IVDD Osteoarthritis Cardiovascular disease Clinical Insight:In Beagles, obesity is not merely a lifestyle issue—it is a major disease amplifier. 2.3 Clinical Implications of Morphology and Behavior The defining traits of the Beagle—its appetite, ear structure, endurance build, and independent temperament—are direct products of its functional history as a scent hound. However, these same traits also create predictable veterinary risks and management challenges. Table 1. Functional Traits and Associated Clinical Risks in Beagles Trait Functional Role Clinical Risk Strong Appetite Survival advantage; enhances trainability (e.g., detection work such as “Beagle Brigade”) Obesity; dietary indiscretion; foreign body ingestion → gastrointestinal obstruction, toxicity Drooping Ears Trap and funnel scent particles toward the nose during tracking Otitis externa; bacterial (Pseudomonas) and yeast (Malassezia) overgrowth due to reduced airflow Active Tracking Behavior + Body Structure High stamina; low center of gravity supports sustained scent tracking Increased spinal stress → Intervertebral Disc Disease (IVDD); joint strain Independent Temperament Enables autonomous tracking over long distances Training difficulty; poor recall; roaming behavior → environmental hazards (e.g., traffic) 2.3.1 Appetite and Metabolic Risk Beagles exhibit a voracious and indiscriminate appetite, a trait historically advantageous for survival and now leveraged in working roles requiring food-based training. From a clinical perspective, this predisposition results in: High obesity risk, which significantly
Bengal Cats and Breed-Linked Disease Risks: A Clinical Perspective on Genetics, Behavior, and Preventive Care

Table of Contents 1. Introduction: A Hybrid Breed with Distinct Clinical Implications The Bengal cat is a domesticated breed developed through hybridization between domestic cats—most notably the Egyptian Mau and Abyssinian—and the Asian leopard cat (Prionailurus bengalensis). This lineage does not merely produce an exotic phenotype; it establishes a distinct physiological, behavioral, and clinical profile that directly influences how the breed should be managed in veterinary practice. From a morphological standpoint, Bengals are long, muscular, and medium- to large-sized, with a broad head, pronounced whisker pads, high cheekbones, and wide, expressive eyes accentuated by characteristic periocular markings. Their physicality reflects what is often described as the “grace of a jungle cat”—a combination of stealth, agility, and explosive movement. However, in clinical terms, these traits are not superficial; they are indicative of heightened metabolic demand, neuromuscular activity, and behavioral intensity. Behavioral Demands and Stress-Linked Clinical Expression In practice, Bengal cats consistently demonstrate exceptionally high cognitive and physical requirements. Unlike typical domestic breeds, they require sustained environmental engagement—often 30 to 60 minutes of structured interactive activity daily, in addition to access to vertical climbing environments that accommodate their arboreal instincts. Failure to meet these requirements is not benign. Chronic understimulation frequently manifests as stress-mediated pathological behaviors, including: Pica: Ingestion of non-nutritive materials, increasing the risk of gastrointestinal obstruction Psychogenic Alopecia: Excessive grooming resulting in alopecia and secondary dermatologic complications Inappropriate Elimination: Litter box aversion or urine marking driven by environmental or territorial stress From a clinical perspective, these presentations are often misinterpreted as isolated behavioral issues, when in fact they represent environmental mismatch syndromes—a mismatch between innate behavioral programming and domestic living conditions. Genetic and Systemic Disease Predispositions Despite their robust appearance, Bengals carry a predictable set of inherited and breed-associated disorders, many of which remain subclinical until advanced stages: Hypertrophic Cardiomyopathy (HCM): A primary myocardial disorder characterized by left ventricular hypertrophy. It is a leading cause of morbidity and mortality, often progressing silently until complications such as congestive heart failure or Feline Aortic Thromboembolism (FATE) occur—manifesting as acute hind limb paralysis. Progressive Retinal Atrophy (PRA-b): A recessively inherited condition unique to the breed, resulting in early-onset photoreceptor degeneration and eventual blindness, frequently by two years of age. Pyruvate Kinase Deficiency (PK-Def): A metabolic disorder affecting erythrocyte survival, leading to intermittent hemolytic anemia, lethargy, and variable clinical severity. Flat-Chested Kitten Syndrome (FCKS): A developmental thoracic deformity observed in neonates, which may compromise cardiopulmonary function depending on severity. These conditions underscore a critical principle: phenotypic vitality does not equate to genetic resilience. Orthopedic Vulnerabilities in a High-Performance Breed The Bengal’s athleticism—characterized by frequent jumping, climbing, and rapid directional movement—places sustained mechanical stress on joints. Clinically, this correlates with an increased incidence of: Patellar Luxation Hip Dysplasia While these conditions may initially be subclinical, progressive joint instability leads to chronic inflammation, cartilage degradation, and osteoarthritis, particularly in aging individuals. Early detection and weight management are therefore essential components of long-term care. Anesthetic and Pharmacological Sensitivities From a pharmacological standpoint, Bengals require heightened caution in anesthetic protocols. Clinical reports and practitioner experience indicate increased sensitivity to certain agents, particularly ketamine. Adverse responses may include: Dysphoric or prolonged recovery Neuromuscular hyperactivity Hyperthermia Cardiovascular instability This sensitivity is hypothesized to be linked to variations in hepatic Cytochrome P450 enzyme activity, affecting drug metabolism and clearance. Consequently, individualized anesthetic planning and vigilant perioperative monitoring are strongly advised. Nutritional Considerations and Metabolic Demand The Bengal’s high lean muscle mass and activity level translate into elevated metabolic requirements compared to typical indoor cats. Optimal nutritional strategies include: High-protein diets (approximately 45–55% dry matter) Moderate-to-high fat content to sustain energy expenditure Supplementation with: Omega-3 fatty acids (anti-inflammatory support) Glucosamine and chondroitin (joint health) Inadequate nutritional alignment may exacerbate both musculoskeletal strain and systemic health vulnerabilities. Clinical Framing Collectively, these factors position the Bengal cat not simply as a visually distinctive breed, but as a high-performance companion animal with specialized medical and environmental requirements. In clinical practice, the Bengal should be approached not as a standard domestic cat, but as a genetically and behaviorally distinct population requiring proactive, precision-based care strategies. 2. Coat, Phenotype, and Selective Breeding Pressure The Bengal’s defining visual identity—its sharply contrasted spotted (rosetted) or marbled coat—represents one of the most intensively selected phenotypes in companion animal breeding. Achieving this “wild-type” aesthetic while preserving a manageable domestic temperament has required sustained, high-pressure selective breeding within a relatively narrow genetic pool. From a clinical genetics perspective, this process provides a clear illustration of how phenotypic refinement can reshape population-level health risk. 2.1 The Genetics Behind the Bengal Phenotype Contrary to common perception, the Bengal’s exotic coat is not solely derived from its wild ancestor. Recent genetic analyses indicate that: Many defining coat traits originate from domestic cat gene variants, which were selectively amplified Wild Asian leopard cat DNA contributes to pattern framework, but not all visible traits Notable examples include: “Glitter” phenotype: A highly prized trait producing a soft, iridescent sheen. This is associated with mutations in the Fgfr2 gene, originating from domestic cat lineages rather than the wild progenitor. “Charcoal” pattern: A darker, high-contrast phenotype resulting from genomic interaction (incompatibility) between the leopard cat’s Asip gene and domestic alleles—highlighting the complex interplay between hybrid genomes. Clinical interpretation: These traits are not biologically neutral. They are the result of targeted allele fixation, often achieved at the expense of broader genetic variability. 2.2 The Clinical Cost: Amplification of Inherited Disease The same selective pressure that stabilizes desirable coat traits also increases the probability of co-inheriting deleterious mutations, particularly within a restricted breeding population. This manifests most clearly in autosomal recessive and heritable conditions, where asymptomatic carriers propagate disease alleles across generations. Autosomal Recessive Disorders Progressive Retinal Atrophy (PRA-b): A breed-specific, recessively inherited condition leading to early-onset blindness. Large-scale screening studies have demonstrated carrier rates of approximately 18% in European Bengal populations, underscoring the risk of silent transmission in the absence of DNA testing. Pyruvate Kinase Deficiency (PK-Def): A metabolic disorder affecting erythrocyte survival, resulting in intermittent hemolytic anemia. This mutation
Feline Pancreatic Lipase
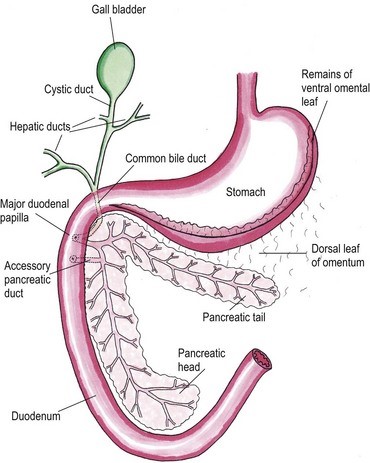
Feline Pancreatic Lipase LIN, WEN-YANG (WESLEY), Ph.D Feline Pancreatic Lipase is a powerful diagnosing biomarker for feline pancreatitis, whereas serum amylase and serum lipase are usually used in diagnosing pancreatitis for canine, are not effectively in detecting pancreatitis for cats. Anatomical physiology function of pancreas in cats The feline pancreas is a digestive glandular organ, which presents a long v-shaped strip of configuration locating at abdomen between stomach and duodenum. The tail part of feline pancreas rests toward the dorsal extremity of the spleen and connect to mesocolon with omentum (Figure 1). Figure 1. Anatomic view of the pancreas and its surrounding tissues https://veteriankey.com/pancreas-4/ The normal pancreas colored on pale pink and perform both functions of endocrine and exocrine. The endocrine portion contains small clusters of pancreatic α- and β-cells within Langerhans (approximately 2% of the gland’s weight) that majorly generates two hormones proteins: glucagon and insulin. Glucagon works to elevate the level of blood sugar, whereas insulin would diminish excess circulating blood sugar. Both of glucagon and insulin would take part in regulating homeostasis of glycemic level. Acinar and ductal cells are major members in the exocrine portion of pancreas. Acinar cells aggregate around the terminal pancreatic ductules to secrete digestive enzymes include trypsinogen, chymotrypsinogen, proelastase, procarboxypeptidase, ribonucleases, deoxyribonucleases, phospholipase A2, carboxylesterase amylase and lipase. Amylase and lipase are contributing to hydrolyze carbohydrates and fat. Others may play roles as proteases to cleave polypeptide chains. Feline’s ductal cell generates antibacterial proteins to protect small intestinal from bacterial infection. Moreover, ductal cell can also produce bicarbonate and water for neutralizing pH in the duodenum. Intrinsic factor such as vitamin B12 would be made from ductal cell too. The pancreas is the only generating organ of intrinsic factor for feline, whereas dogs could produce intrinsic factor from pancreas and stomach. All pancreatic enzymes would secret into small intestine for digesting fats, proteins and carbohydrates. Furthermore, the abnormal seep of exocrine enzymes to pancreas and its surrounding organs could cause pancreatic inflammation known as pancreatitis. The highest occurrence of feline pancreatic diseases is exocrine pancreatic insufficiency (EPI) and pancreatitis. Pancreatitis in the cat Feline pancreatitis is classified as acute (temporary morphological changes) and chronic (permanent morphological change) type according to the condition of histopathologic changes after treatment. Acute necrotizing pancreatitis (ANP) and acute suppurative pancreatitis are two of the most common types of acute feline pancreatitis, whereas chronic non-suppurative pancreatitis (CP) and pancreatic atrophy are chronic conditions. Common acute pancreatitis in feline would show anemia, leukocytosis, hypokalemia, hypocalcemia, hyperglycemia, elevation of ALT, ALP, total bilirubin, cholesterol and decreasing level of albumin. Acute necrotizing pancreatitis (ANP) usually present pancreatic acinar cell necrosis, peripancreatic fat necrosis followed inflammation, hemorrhage, mineralization and fibrosis. Despite of its idiopathic character, several diseases have considered to be related with development of ANP including concurrent biliary tract disease, ischemia, pancreatic ductal obstruction, toxoplasmosis, feline Herpes virus infections, feline infectious peritonitis, pancreatic fluke infestations (Eurytrema procyonis, Amphimerus pseudofelinus), trauma, organophosphate poisoning and hepatic lipidosis. General anesthesia induced hypotension or surgical venous outflow occlusion would decrease pancreatic blood flow and cause ANP. Acute suppurative pancreatitis is less common than ANP in feline and neutrophilic inflammation would happen with it. Besides, the continuous and progressive inflammatory process of the pancreas would lead to chronic non-suppurative pancreatitis (CP) in which lymphocytic inflammation, fibrosis, and acinar atrophy are the major features. The end stage of CP in most feline cases would usually result in pancreatic atrophy, which may or may not influence the endocrine portion of the gland. Felines who suffer pancreatic atrophy would occur cobalamin and fat-soluble vitamin malabsorption, severe maldigestion, acid injury in duodenal mucosa, and bacterial proliferation in the gut due to exocrine pancreatic insufficiency. Since various types of pancreatitis such as acute and chronic pancreatitis, pancreatic abscess, pancreatic cyst/pseudocyst, exocrine pancreatic insufficiency, and neoplasia share overlapping symptoms, thus histopathology cab be used to discern different conditions. Symptoms of feline pancreatitis Symptoms of feline pancreatitis would occur lethargy, anorexia, dehydration, hypothermia, vomiting, weight loss, Jaundice, cholangiohepatitis, hepatic lipidosis, biliary obstructions, cranial abdominal masses and cranial abdominal discomfort. Besides, hepatic and intestinal disease would concurrent. I. Acute feline pancreatitis: Vomiting, poor appetite, poor activity, diarrhea, abdominal pain, drooling, fever, collapse. II. Chronic feline pancreatitis: Frequent vomiting, poor appetite, listless, frequent diarrhea, abdominal pain, drooling, fever, collapse, hypothermia, breathing too fast or too slow, fast heartbeat. Possible Causes of feline pancreatitis Scientists presumed that premature trypsin activate of digestive zymogens in pancreatic acinar cells would cause pancreatic autodigestion, acinar cell necrosis, hemorrhage, and fat necrosis, saponification, mast cell degranulation, leukocyte chemotaxis, platelet aggregation, vasodilation, surfactant degradation within the lungs and initiation of disseminated intravascular coagulation (DIC) for worse cases. Diagnosis and general considerations Since symptoms of feline pancreatitis were similar to common flu, vets probably can’t judge it correctly at the early stage without proper diagnostic tools. It’s not an easy task to diagnose pancreatic disease within cats. Single diagnostic method is not recommended. The diagnosis of feline pancreatitis relied on combinational diagnostic tools include historical data, physical examination results, laboratory, and Bio-imaging. Especially, histopathology plays the role as the definitive conclusion for feline pancreatitis. Middle-aged felines are susceptible to pancreatitis; whereas, older felines (mean 12.8 years, range 4–20 years) are susceptible to neoplasia, cyst/pseudocysts. Diagnostic imaging Radiography, computed tomography (CT) and ultrasonography were effective imaging tools applied in diagnosing feline pancreatitis. Among all imaging tools, ultrasonography is the most reliable imaging modality for the diagnosis of feline pancreatic diseases, which can help identify soft tissue masses, cysts/pseudocysts, abscesses, or neoplasia and lesions of feline pancreatitis. Clinicopathologic tests The general clinicopathologic test for feline pancreatitis include complete blood cell count, serum bilirubin, cholesterol, glucose, total protein, albumin, and serum activity of liver enzymes (serum alanine aminotransferase and alkaline phosphatase), calcium, urea, creatinine, and potassium. However, serum lipase and amylase activities can’t be diagnostic indicator for feline pancreatic disease. Nevertheless, feline trypsin-like immunoreactivity (fTLI) and